- Visibility 211 Views
- Downloads 32 Downloads
- DOI 10.18231/j.jsas.2020.007
-
CrossMark

Application of magnets in orthodontics –A review
Introduction
Magnetic force is an essential ingredient of nature. Magnets have generated great interest within dentistry. They have been used for various applications in orthodontics and prosthodontics. Earlier use of magnets was limited due to the unavailability of small size magnets, but after the introduction of rare earth magnets and their availability in smaller sizes, their use has increased considerably.[1] The force they deliver can be directed, and they can exert their force through mucosa and bone as well as within the mouth. [2], [3] In orthodontics, they are used for intrusion of teeth, tooth movement along archwires, expansion, retention, in functional appliances and in the treatment of impacted teeth. [4], [5], [6], [7] There are various types of magnets used in the field of orthodontics with their advantages and disadvantages, along with their biological safety which has been discussed in this article. This article reviews various uses of magnets in the field of orthodontics.
Physical Properties of Magnets
All magnets have magnetic fields around them. The field emerges from one pole of the magnet conventionally known as ‘N’ pole and goes to other pole that is ‘S’ pole. Magnetic field can be either Static or Time varying.
Coulomb’s Law
All magnets obey this law which states that ‘force between two magnetic poles is proportional to their magnitudes (M) and inversely proportional to the square of the distance between them.’
F=Md2
The rare earth magnets give maximum force at short distance in comparison to elastics, which attain maximum force at more distance.
Curie point
Rare earth magnets tend to loose their magnetism at room temperature. To overcome this in orthodontics it has been combined with other element such as boron so that they can be incorporated into appliances and heat stabilized.
Pierre Curie observed that magnets tend to lose their properties at specific temperature which causes their domain to return to random distribution. This point of temperature is called Curie Point.
Important Intra-Oral Properties
Three dimensional centripetal orientation of attractive magnetic force.
Interruption of magnetic force line by Intermediate media.
No energy loss.
When two magnets are displaced in all the three planes they attract to a complete overlap. Centripetal attraction in all 3 spatial dimensions gives the operator complete teeth control on precise engagement.
Intra oral magnets are attracted to each other even if soft or hard tissues are interspersed in the gap between the two magnets eg: impacted canines.
When compared to elastics which shows force degradation & deteriorate over a short time, the rare earth magnets can maintain constant energy if protected against corrosion, curie temperature etc.
Types of Magnetic Appliances
Platinum Cobalt
Al –Ni-Co
Ferrite
Cr–Co -Fe
Samarium Cobalt
Neodymiun Iron Boron
Rare earth magnets
High cohesive forces that is high resistance to demagnetization
Capable of producing high forces relative to their size due to the property of Magnetocrystaline Anisotropy
Strong permanent magnets made from alloys of rare earth elements. They are substantially stronger than ferrite or alnico magnets.
Anisotropy is the property of substances to exhibit variations in physical properties along different molecular axis.
Samarium Cobalt magnets (SmCo5 & Sm2Co17): Introduced by Becker in 1970. They have Superior magnetic properties compared to other rare earth magnets
Advantages
Force necessary in orthodontics can be obtained from small size of the magnets
High resistance to demagnetization
High Curie point (more stable
High Corrosion resistance
Biologic concept of Magnetic force and Histologic changes
No subcutaneous changes as inflammation or adverse reaction under the magnets
Resorption of bone occurred under magnets after 3-4 weeks
Reduced chances of necrosis of bone as magnets make erythrocytes thinner
Magnetic forces inflicted a minimum of stress that induces various bio-chemical changes in a patient during orthodontic tooth movement.
Lars Bondemark & J. Kurol
Studied changes in human dental pulp and gingival tissue on exposure to magnetic field. They found no difference in clinical gingival condition and pulpal condition.
McDonald (1993)
Reported increased proliferation and systemic activity in fibroblasts in presence of static magnetic field
Lars Bondemark & A. Wennberg (1994): Study showed that-
Uncoated Samarium magnets showed severe toxicity
Parylene coated Samarium magnets showed mild toxicity
Coated & uncoated Neodymium magnets showed negligible toxicity
Short term exposure to magnet fields did not cause any cytotoxic effect on cells
Application of magnets in orthodontics
Orthopedic
Expansion of arch
Growth modulation- Class II correction with functional appliances (eg; Magnetic Twin block, FOMA)
Orthodontic
Fixed mechanotherapy- extraction & non-extraction
Relocating impacted teeth
Distal/mesialization of molars
Intrusion of posterior teeth in open bite cases
Closure of diastema
Uprighting and Derotation of teeth
Magnetic Brackets
Magnetic appliance for treatment of snoring in patients with and without sleep apnea
Extrusion of fractured teeth
Retainers (micro magnetic retainer)
Magnetic Appliances- Magnetic forces are used to bring about orthodontic tooth movement, Derived from magnets in attraction or repulsive mode
Advantages
Eliminates patient co-operation
Less pain and discomfort
Continuous force = reducing treatment time
Reduced periodontal disturbance, root resorption & caries
No friction & Better directional force control
Less chair side time
Disadvantages
Tarnish & corrosion
Cytotoxic effects
Bulk
Bitter Taste
Expensive
Appliances & other orthodontic uses of magnets
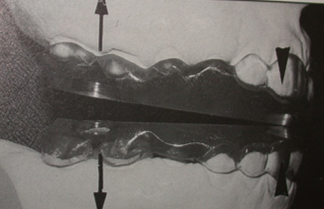
Active Vertical Corrector (AVC)
Developed by Dellinger in 1986, as a non surgical alternative treatment for Skeletal open bite
Can be fixed/removable and works as an energized bite block.
As it is energized only by the intermittent force from the muscles of mastication—electromagnetic field.
Superior to static bite block appliance
The energy system is obtained by the repelling force of Sm-Co magnets encased in a stainless steel capsule.
Constant force system results in rapid tooth movement than conventional appliances such as high-pull headgear, Activator bite block therapy.
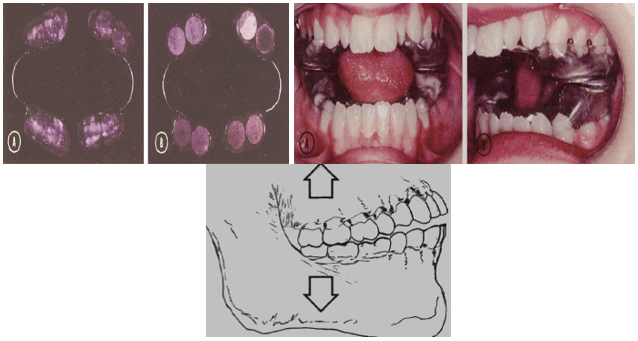
Mechanism of Action
Reciprocal intrusion of maxillary and mandibular teeth resulting in autorotation of mandible and open bite correction
Activation
Intermittent force from the muscles of mastication leads to activation of electromagnetic field which leads to increase in remodeling and finally orthodontic tooth moement.
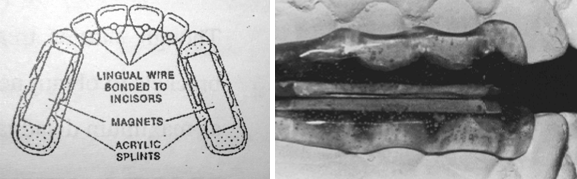
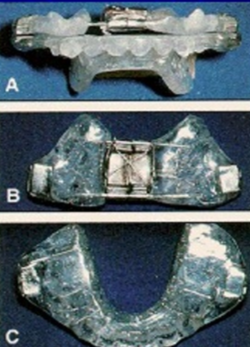
Fixed Magnetic Appliance
Introduced by Varun Kalra & Charles Burstone in 1989.
Used for Growth modulation.
Appliance has the repelling SmCo magnets embedded in the upper and lower acrylic splints.
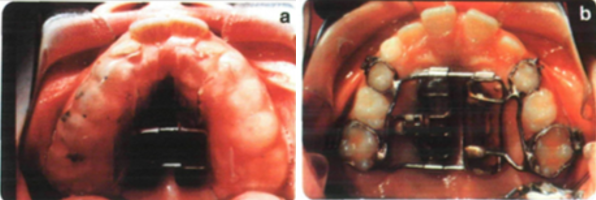
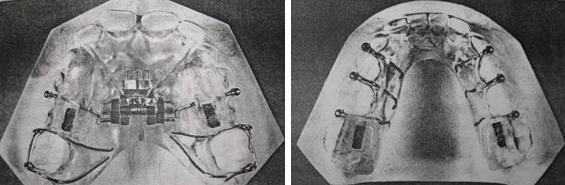
Expansion
Vardimon and Graber (1987) demonstrated palatal expansion using two types of appliances
Advantages
Physiologic forces
Avoids the rotation of maxilla
Disadvantages
Expansion is slower.
Bulky, needs stabilization
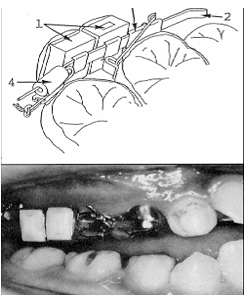
Tooth Impaction
Vardimon, Graber, Drescher (1991) used Nd2Fe14B magnets to assist eruption of an impacted canine.
Procedure:-A mucoperiostal flap is raised uncover impacted canine — Vertical magnetic bracket/small magnet are bonded to the lingual crown surface.
The Force acts through a bigger intra oral magnet placed in removable appliance.
Advantage: simple, frictionless, short treatment time

Magnets for diastemas (Muller (1984))
Rectangular SmCo magnets
Light continuous forces
Direct bonding to the labial aspect of the tooth.
Advantages
No archwires
Less Chair side time
Position of teeth can be controlled by position of magnets

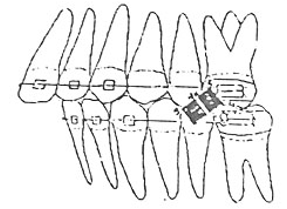
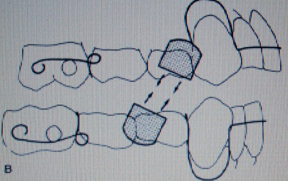
CL-II mechanics in extraction cases
Upper magnet - attached to the upper sectional arch & ligated to mesial aspect of canine
Lower magnet- attached to lower sectional arch
Upper & lower magnetic poles in attraction result in tooth movement
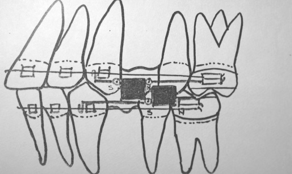
CL-II mechanics in non-extraction cases
Upper magnet - mesial to molar tube
Lower magnet -mesial to the upper magnet
At 700 from the horizontal plane
0% air gap for Maximum force
Magnets in attraction or repulsion can be used to drive upper buccal segment distally.
Molar distalization (Gianelly(1988))
Two repelling magnets for each maxillary quadrant.
Nance appliance is placed to reinforce the anchorage.
Constant force = 80z
Bondemark & Kurol (1994)
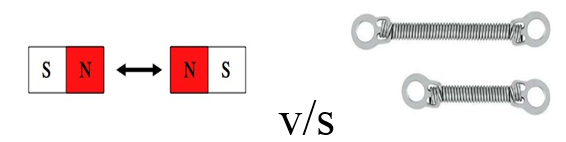
Results: Coil are most comfortable & forces were more constant than magnet forces.
Disadvantage of magnets
Difficulty in correctly positioning
Risk of swallowing if dislodged
Magnetic edgewise brackets
Introduced by Kawata (1987),
Shorter treatment time & good biocompatibility.
But of lab procedure is complex
Chromium plated SmCo magnets soldered to base of edgewise brackets which were directly bonded to the teeth

Functional Orthopedic Magnetic Appliances (FOMA)
(Vardimon et al (1989))
Developed FOMA for correction of Class II & III malocclusions
It had shown positive treatment effects in monkeys
FOMA II (NeFeBo)
It has upper and lower attracting magnets.
Active appliance, directs its inherent magnetic forces to the jaws, thereby keeping the jaw in an advanced posture.
FOMA III (Ne-Fe-Bo)-
The upper magnet is attached to a retraction screw, the lower magnetic housing is attached near the lingual surface of the central incisors.
The upper magnet is retracted periodically to stimulate maxillary advancement and mandibular retraction.
FOMA III has a biphasic action-
Immediate rapid sutural Expansion
Slow and delayed cartilaginous suppression.

Magnetic activator device
Developed by Darendilier (1993)
MAD I – used for correction of mandibular deviation
MAD II – for Cl II corrections
This removable appliance postures the mandible forward.
Attractive force was about - 600 gms.
Cl-II malocclusion corrected by posterior movement of upper jaw and forward movement of mandible.
First 6 months – full time.
Next 2 months – night time only.
It consists of an upper and lower Hawley’s framework carrying a rectangular magnet in premolar region.
Mad III
MED + MAD III for early treatment of Class III malocclusion.
Maxillary expansion and stimulation of forward maxillary growth, to obtain dental and skeletal correction
MAD IV - open bite correction
It consists of anterior attracting magnets and posterior repelling NeFeBo magnets.
The repelling magnets generate a force of 300g.
Anterior magnets guides mandible into a centered midline position and enhance anterior rotation of mandible.
The Propellant Unilateral Magnetic Appliance (PUMA)
Treatment of hemifacial microsomia by Chafe (1995)
Repelling SmCo magnets in U/L acrylic bite blocks
Simulates autogenous costochondral graft
In these individuals there is underdevelopment of one half of the facial structures and muscles on the affected side.

Magnetic twin block (Clark (1996))
• SmCo magnets are embedded in the inclined surface of the twin block in attraction mode.
Extrusion of fractured teeth
McCord & Harvie (1984) & Bondemark & Kurol (1997) used magnets to extrude teeth with fractured roots.
Attractive magnets - one at root fragment & other in removable appliance.
After the desired extrusion the tooth can be restored
Micro Magnetic Retainers
Springate & Sandler(1991)
Micro magnets made of Ne-Fe-Bo can be used as fixed retainer in patients with midline diastema.
More physiologic tooth movement and better oral hygiene

Recycling of magnets
Bondemark & Kurol conducted extensive studies on recycling (autoclaving) of rare earth magnets.
Biocompatibility, force & stability is not effected
Darendililer - magnets should not be recycled for ethical reasons & also to prevent demagnetization
Discussion
Early attempts at using magnets for intraoral uses were unsuccessful, mainly because of the large size of magnets at that time and the inadequate forces that they provided. However, since the introduction of rare earth magnets, such as samarium-cobalt and neodymium-iron-boron, it has become possible to produce magnets with small enough dimensions to be used in dental applications and still provide the necessary force. Introduction of rare earth magnets into orthodontics for various therapeutic uses is very recent. Within 10 years, magnetic forces have gained good acceptance in correction of skeletal and dental defects. The main advantage with magnets is operator controlled. It eliminates patient cooperation. Conceivable risks of harmful biological effects are negligible with magnets. It is easy to maintain oral hygiene. Compared with other conventional orthodontic methods of force delivery systems magnets are cost effective. Their high cost can overcome by reusing it after sterilization and recycling. These magnets after recycling have not shown much change in their force system. Magnets suffer from tarnish and corrosion. Tarnish and corrosion products are cytotoxic. Tarnish and corrosive nature is prevented by casing them in stainless steel jackets (or) giving parylene coat. Magnets exert continuous forces with less friction, compared to other conventional orthodontic appliances. Teeth movement are bodily in nature and treatment time is shorter. They can be associated along with fixed, removable and functional appliances. Uses of extraoral forces are minimized and anchorage control with them is very precise. Magnets can be used to give predictable forces in either attraction or repelling mode. The orthodontic stimuli provided by the magnetic appliance have reduced the systemic stress reaction seen with conventional orthodontic mechanotherapy. The incidence of periodontal disturbances, root resorption and caries are considerably low and foremost no discomfort.
Conclusion
Superiority of results with magnetic appliances as compared to those of conventional orthodontic appliances is still in dispute. The evidence currently suggests that the risk of harmful biological effects are negligible. High cost can be overcome by reusing after sterilization & recycling.
Source of Funding
None.
Conflict of Interest
None.
References
- A D Vardimon, T M Graber, D Drescher, C Bourauel. Rare earth magnets and impaction. Am J Orthod Dentofacial Orthop 1991. [Google Scholar]
- V S Bhat, K K Shenoy, P Premkumar. Magnets in dentistry. Arch Med Health Sci 2013. [Google Scholar]
- S J Behrman. The implantation of magnets in the jaw to aid denture retention. J Prosth Dent 1960. [Google Scholar]
- L Bondemark. Long-term effects of orthodontic magnets on human buccal mucosa - a clinical, histological and immunohistochemical study. Eur J Orthodon 1998. [Google Scholar]
- S. D. Springate, P. J. Sandler. Micro-magnetic Retainers: An Attractive Solution to Fixed Retention. Br J Orthodon 1991. [Google Scholar]
- T Kawata, K Hirota, K Sumitani, K Umehara, K Yano, H J Tzeng. A new orthodontic force system of magnetic brackets. Am J Orthodon Dentofac Orthoped 1987. [Google Scholar]
- M G Woods, R S Nanda. Intrusion of posterior teeth with magnets. An experiment ingrowing baboons. Angle Orthod 1988. [Google Scholar]
- Introduction
- Physical Properties of Magnets
- Coulomb’s Law
- Curie point
- Important Intra-Oral Properties
- Types of Magnetic Appliances
- Rare earth magnets
- Advantages
- Biologic concept of Magnetic force and Histologic changes
- Lars Bondemark & J. Kurol
- McDonald (1993)
- Lars Bondemark & A. Wennberg (1994): Study showed that-
- Application of magnets in orthodontics
- Orthopedic
- Orthodontic
- Advantages
- Disadvantages
- Appliances & other orthodontic uses of magnets
- Active Vertical Corrector (AVC)
- Fixed Magnetic Appliance
- Expansion
- Advantages
- Tooth Impaction
- Magnets for diastemas (Muller (1984))
- CL-II mechanics in extraction cases
- CL-II mechanics in non-extraction cases
- Molar distalization (Gianelly(1988))
- Bondemark & Kurol (1994)
- Magnetic edgewise brackets
- Functional Orthopedic Magnetic Appliances (FOMA)
- Magnetic activator device
- The Propellant Unilateral Magnetic Appliance (PUMA)
- Magnetic twin block (Clark (1996))
- Extrusion of fractured teeth
- Micro Magnetic Retainers
- Discussion
- Conclusion
- Source of Funding
- Conflict of Interest