- Visibility 168 Views
- Downloads 46 Downloads
- Permissions
- DOI 10.18231/j.jsas.2021.013
-
CrossMark

Abstract
Background: Acute pancreatitis has multiple aetiologies. Acute pancreatitis is divided into interstitial oedematous pancreatitis or necrotizing pancreatitis based on morphology. According to the revised Atlanta classification necrotizing pancreatitis is further subdivided into acute necrotic collection if the disease develops within 4 weeks or walled-off necrosis if the disease develops after 4 weeks.
Case Presentation: We report a case of 40years male, with acute pancreatitis for 1 month, presenting with decreased appetite, loss of weight, and tremors of extremities. CT featured active necrotizing pancreatitis with peripancreatic necrosis, collections, and superadded infection which was drained by percutaneous pigtail catheter.
Discussion: Percutaneous pigtail insertion controls the symptoms and this procedure is effective in the management of patients with necrotizing pancreatitis. It serves as definitive or intermediate therapy to surgical necrosectomy in patients who are unfit for surgery. Percutaneous pigtail insertion can be done following a peritoneal or retroperitoneal approach4, both approaches have different advantages and it is the choice of the radiologist and the location of the residual collections. The disadvantages are duct leak and it needs multiple check CT’s but in well trained and experienced hands the disadvantages are minimized.
Conclusion: Percutaneous pigtail insertion is an alternative approach in the management of necrotizing pancreatitis when the patient is seriously ill or unfit for surgery. It can prevent life-threatening complications and it can be considered as a primary modality in treating a patient with walled-off necrosis.
Key Messages: Percutaneous pigtail insertion an alternative approach in the management of necrotizing pancreatitis when the patient is seriously ill or unfit for surgery can be considered as the primary modality of choice in treating patients with walled-off necrosis of the pancreas.
Introduction
Acute pancreatitis is an inflammatory condition of the pancreas which is characterized by severe epigastric abdominal pain radiating to the back and elevated levels of pancreatic enzymes in the blood.[1] Several aetiologies contribute to acute pancreatitis. Of these, gallstones, chronic alcohol use disorders are more common.[2]
Acute pancreatitis can be divided into interstitial oedematous pancreatitis or necrotizing pancreatitis. According to the revised Atlanta classification necrotizing pancreatitis is further subdivided into acute necrotic collections if the disease develops within 4 weeks or walled-off necrosis if the disease develops after 4 weeks.[3] Management of acute pancreatitis can be conservative, surgical or interventional.
Major complication of pancreatic necrosis is formation of abscess with gas. Another complication is disconnected main pancreatic duct. Disconnection occurs when a segment of the pancreatic ductal epithelium undergoes necrosis and viable pancreatic tissue becomes isolated from the duodenum. It may lead to continuous leak with consequent inflammation and infection.
Here, we present a case of acute necrotizing pancreatitis with parenchymal and peripancreatic necrosis along with collections as per CT abdomen findings. The patient was managed by CT guided Pig tail insertion. This was opted to avoid complications of surgery and post-operative surgical complications. The aim of this study is to adopt a simple life saving radiological procedure as the management option for acute necrotizing pancreatitis with collections and to consider dual Pigtail drainage as the first line of management.
Case Presentation
A 40-years male, presented to Kasturba Medical College, Attavar, Mangalore with the history of acute pancreatitis for the past 1 month now he has loss of weight, loss of appetite and tremors involving the hands and feet. He is a known hypertensive and diabetic. No previous history of any surgeries.
On clinical examination, he was found to be afebrile with normal vitals and unremarkable general physical examination. Abdomen was distended with diffuse tenderness. Haematological investigations showed leucocytosis and lymphopenia. Biochemical examination showed normal amylase and lipase levels.
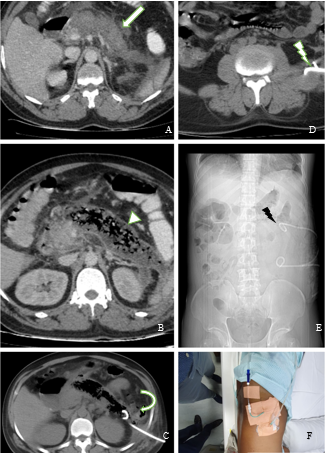
Contrast enhanced CT abdomen was done on intervals which revealed
[Figure 1] A. Enlarged heterogenously enhancing pancreas with extensive fat stranding and peripancreatic fluid collections (White arrow). Another contrast enhanced CT abdomen performed 3 weeks later revealed [Figure 1] B. Active narcotizing pancreatitis with pancreatic parenchymal, peripancreatic necrosis with a large necrotic collection with superimposed air foci-suggestive of super added infection (arrow head).
As a temporary management at this stage drainage of the collections was facilitated by CT guided Pig tail insertion.Under local infiltrative anaesthesia pigtail catheter 12 Fr was introduced from the left 10-11 intercostal space. Check CT was done to confirm the location of the pig tail ([Figure 1] C) (Curved Arrow). It was found well positioned and collection were drained and the same was sent for culture and sensitivity and biochemical measurement of pancreatic enzymes (Lipase, Amylase).
A week later another pig tail of same size was inserted lateral to the left lumbar region into left parapsoas region for the purpose of draining the dependent collections. ([Figure 1] D, E) (Thunder arrow)
Two pig tail’ s was considered because one pig tail can be used to flush the area with normal saline and the other pig tail to drain out the collections. First pigtail insertion was by peritoneal approach and later was by retroperitoneal approach. A month later another CT was done which showed significant reduction in the residual collection
Patient tolerated both the procedures well and the postprocedure period was uneventful. Patient recovered well.
Discussion
Imaging-guided bridging approach for the management of necrotizing pancreatitis includes fine-needle aspiration, catheter drainage of collections. According to the American College of Radiology appropriateness criteria with radiological imaging suggesting a liquefied drainable collection, enlarging collections, collections > 5 cm, collections causing obstruction and infected collections.[4] As per this criterion percutaneous pig tail insertion was done which helped the patient to control the symptoms of necrotizing pancreatitis (sepsis, inability to tolerate feeding) as in our case. It represents definitive therapy or serve as bridging therapy in a “step-up” approach to surgical necrosectomy. It is the therapeutic option for patients unfit for surgery. It is also used to treat residual collections post necrosectomy. We followed both the peritoneal and retroperitoneal approach in draining the collection[5] and for giving symptomatic relief to the patient. It served as a definitive therapy to our patient with walled off necrosis both the approaches have different advantages and it is the choice of the radiologist and the location of the collections. Disadvantages of Pigtail insertion is duct leak and it needs check CT scans in the region of interest (maximum 3). Complications of open necrosectomy outweighs that of percutaneous pig tail insertion.
Conclusion
The above case with necrotizing pancreatitis with collection was drained and treated conservatively using percutaneous pig tail insertion under CT guidance which was considered was the permanent modality for this patient and he recovered well. This is an alternative approach to surgical necrosectomy in the management of necrotizing pancreatitis it can prevent life threatening complications and it can be considered as a primary modality in treating a patient with walled off necrosis.
Source of Funding
None.
Conflict of Interest
None.
References
- Ralston SH, Penman ID, Strachan M. Davidson's Principles and Practice of Medicine. . 2018. [Google Scholar]
- Baron TH, Morgan DE. Acute Necrotizing Pancreatitis. New Engl J Med. 1999;340(18):1412-7. [Google Scholar] [Crossref]
- Foster BR, Jensen KK, Bakis G, Shaaban AM, Coakley FV. Revised Atlanta Classification for Acute Pancreatitis: A Pictorial Essay. Radiographics. 2016;36(3):675-87. [Google Scholar] [Crossref]
- Shyu JY, Sainani NI, Sahni VA, Chick JF, Chauhan NR, Conwell DL. Necrotizing Pancreatitis: Diagnosis, Imaging, and Intervention. RadioGraphics. 2014;34(5):1218-39. [Google Scholar] [Crossref]
- Sharma P, Sharma S, Yadav A, Rotem E. CT guided percutaneous drainage in necrotizing pancreatitis - highly successful in appropriately selected patients - single center experience. J Pancreas. 2019;20(1):24-9. [Google Scholar]