- Visibility 64 Views
- Downloads 10 Downloads
- DOI 10.18231/j.jsas.2020.016
-
CrossMark

Duplication of infrarenal IVC-a rare developmental anomaly detected on MDCT angiography-Case report
Introduction
Embryogenesis of the IVC is a complex process involving the formation of several anastomosis between three paired embryonic veins. The result of which is numerous variations in the basic venous plan of the abdomen and pelvis. Duplication of infra-renal IVC is a rare congenital anomaly in the development of IVC which can remain undetected throughout life. Duplication of IVC is most commonly detected on autopsy specimens or may be incidentally diagnosed on MDCT angiography during routine scanning for diagnostic workup or preoperative analysis of prospective renal donors.[1] The workup of a living kidney donor includes a CT angiogram to evaluate arterial and venous anatomy, can detect this condition. The discovery of a duplicated IVC on pre-operative imaging of renal transplant patients is of surgical importance as this anomaly can shorten the length of renal vein available to the recipient team and may lead to intra and post-operative complications.[2]
Case Report
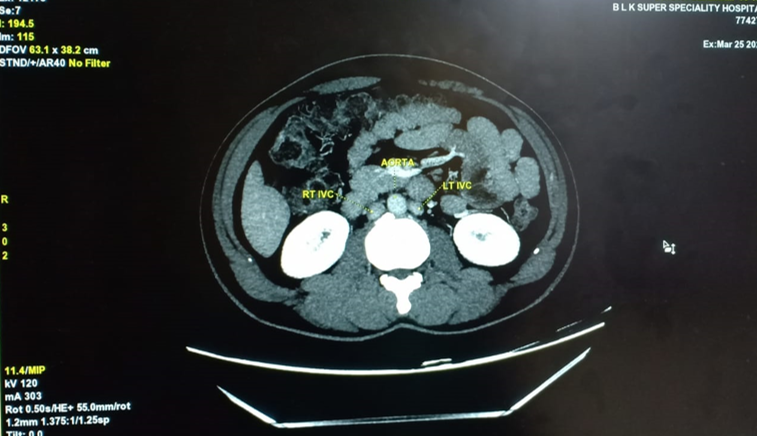
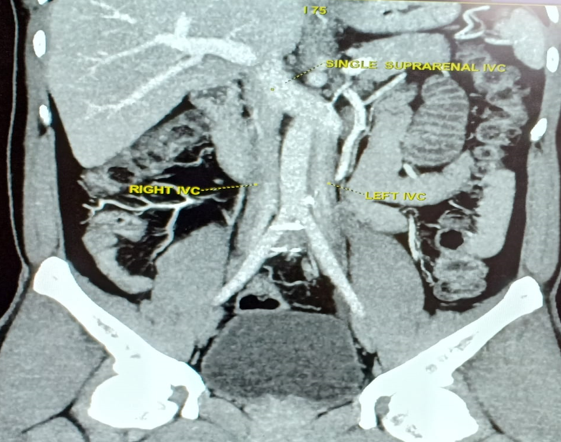
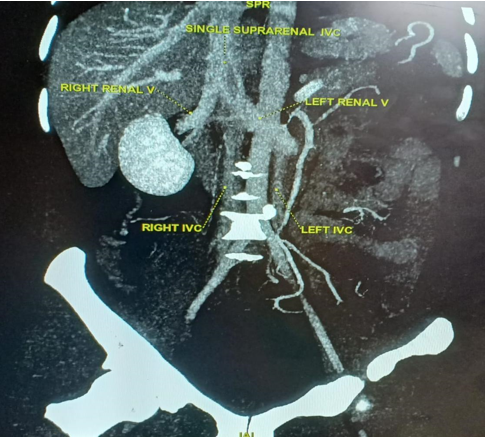
A 33 year old male presented as a prospective renal donor to the Radiodiagnosis department of BLK superspeciality hospital, Pusa road, New Delhi, underwent MDCT angiography scan for the anatomical and vascular evaluation of his reno-vascular system. On MDCT in the late arterial and venous phase two infra-renal IVC’s were found which were seen as a continuation of common iliac veins. The two infrarenal IVCs were found on either side of aorta ([Figure 1]) At the level of left renal vein, left infra renal IVC was seen crossing the midline in front of aorta and joining the right sided IVC to form the suprarenal common trunk ([Figure 2]) and had the normal course and draining vessels thereafter. Right renal vein was seen draining into the common trunk into the suprarenal IVC. Left renal vein was seen draining into the transverse segment of left IVC while crossing the mid line in front of aorta ([Figure 3]). No narrowing or stenosis of any vessel was seen. No other associated anomaly was visualized.
Discussion
The normal IVC is composed of four segments: hepatic, suprarenal, renal, and infrarenal segments. It is derived from a complex embryogenic process beginning at sixth week of gestation and involves three pairs of primitive veins, posterior cardinal, subcardinal and supracardinal veins. Posterior cardinal and subcardinal veins appear and communicate with each other via transverse anastomosis. As the development proceeds two more sets of veins develop which are referred to as supracardinal veins. These supracardinal veins will communicate with the subcardinal veins on the right side via subcardinal-supracardinal anastomosis. The hepatocardiac channel will communicate with the subcardinal vein via subcardinal-hepatocardiac anastomosis. This is the primary arrangement of veins in the developing fetus. As the development proceeds the posterior cardinal veins disappear and similarly the subcardinal veins on each side disappear except for a part of the subcardinal vein extending between posterior cardinal vein and subcardinal-supracardinal anastomosis. With further development, the rest of the veins disappear and the final IVC is formed. The renal segment of IVC develops from the anastomosis between the subcardinal and supracardinal veins, while the hepatic segment of IVC is derived from the right vitelline vein.[3], [4], [5] A duplicated IVC results from persistence of both the right and left supracardinal veins.[6] A left IVC typically ends at the left renal vein, which crosses anterior to the aorta to form a normal right-sided prerenal IVC. In double IVC, the left IVC typically ends at the left renal vein, which crosses anterior to the aorta to join the right IVC.[3] Many classification systems have been proposed for understanding of the different anomalies that may occur during the development of the IVC, however for detailed analysis of the duplicated IVC, some authors have used classification based on the iliac veins. The detection of this vascular anomaly holds significance while operating on the retro peritoneum and it is not uncommon to confuse the left infrarenal IVC with a dilated ureter leading to a life threatening complication.[1] The duplicated inferior vena cava can lead to both, misdiagnosis and to surgical complications in retroperitoneal and aortic surgeries.[7], [8] It also holds ground in renal transplant patients as this anomaly can lead to change in operative planing and avoiding an element of surprise during the procedure. Patients with this anatomical variant are usually asymptomatic. It may increase the risk for development of deep vein thrombosis, especially in young adults due to slow flow, inadequate venous return, and increased venous pressure in the veins of both the lower legs. [9]
Sometimes this anatomical variant is associated with other congenital anomalies or variants. Dudekula et al[1] reported a case where duplicated infrarenal ivc was associated with retrocaval ureter. Saha et al[10] reported rare type of combination of three congenital malformations that is Duplication of IVC, crossed fused kidney and malrotation of gut.
Multidetector CT technolology is the preferred modality for demonstrating the congenital vascular anomalies because of its high spatial and temporal resolution and more so the technique is non invasive and cost effective. It is also valuable in its post processing capabilities in which data can be visualized in 2D or 3D mode providing a clear view of not only the vascular anatomy but the adjacent structures as well.
Conclusion
Isolated duplication of IVC is a rare developmental anomaly that holds surgical significance and MDCT is an excellent modality in detecting the changed anatomy and thus reducing the scope of surgery related complications.
Source of Funding
None.
Conflict of Interest
None.
References
- A Dudekula, S D Prabhu. A rare case of right retrocaval ureter with duplication of infrarenal IVC. . Case Rep Radiol 2014. [Google Scholar]
- P T Kennealey, R F Saidi, J F Markmann, D S C Ko, T Kawai, H Yeh. Duplicated Inferior Vena Cava-Something to Consider in the Evaluation of a Living-Donor Renal Transplant. Dial Transplant 2009. [Google Scholar]
- J E Bass, M D Redwine, L A Kramer, P T Huynh, J H Harris. Spectrum of Congenital Anomalies of the Inferior Vena Cava: Cross-sectional Imaging Findings. Radio Graphics 2000. [Google Scholar]
- H Chen, S Emura, S Nagasaki, K Kin-ya. Double inferior vena cava with interiliac vein: A case report and literature review. Okajimas Folia Anatomica Japonica 2012. [Google Scholar]
- D Coco, S Cecchini, S Leanza, M Viola, S Ricci, R Campagnacci. Inferior vena cava duplication: incidental case in a young woman. Case Rep Radiol 2016. [Google Scholar]
- A Brochert, T Reynolds. Unusual Duplication Anomaly of the Inferior Vena Cava with Normal Drainage of the Right IVC and Hemiazygous Continuation of the Left IVC. J Vasc Interv Radiol 2001. [Google Scholar]
- K Natsis, S Apostolidis, G Noussios, E Papathanasiou, A Kyriazidou, V Vyzas. Duplication of the inferior vena cava: anatomy, embryology and classification proposal. Anatomical Sci Int 2010. [Google Scholar]
- D Pineda, N Moudgill, J Eisenberg, P DiMuzio, A Rao. An interesting anatomic variant of inferior vena cava duplication: case report and review of the literature. Vasc 2013. [Google Scholar]
- R K Sahoo, P Bahinipati, S K Panda. Unusual variant of infrarenal duplication of inferior vena cava. Int J Health Allied Sci 2016. [Google Scholar]
- P Saha, A Garg, K Sahoo, N Kothari, P Garg. Duplication of inferior vena cava with associated anomalies: a rare case report. J Clin Diagn Res: JCDR 2016. [Google Scholar]