
Introduction
Class III malocclusions are described as a facial dysplasia caused by an imbalance in the mandible's size, shape, and position with respect to the maxilla and/or cranial base.1 Skeletal Class III malocclusion is characterized by mandibular prognathism, maxillary deficiency, or some combination of these two features. The aeitiology of Class III malocclusion can be stated as either genetic or environmental in origin.2, 3
The clinicians face a dilemma while treating a Class III malocclusion. Treatment varies in timing, from early intervention during the pre-pubertal stages of development to intervention after the patient has undergone active growth. The treatment modalities range from dentofacial orthopaedic treatment, to camouflage orthodontic treatment to a combined orthognathic surgical and orthodontic approach.4, 5, 6
In cases of early intervention if the skeletal Class III malocclusion is due to mandibular prognathism, mandibular treatment is used to prevent and direct the development of mandible with chin cap. If the skeletal Class III malocclusion is due to maxillary retrognathism, maxillary protraction treatments are performed with use of facemask.
The aim of using a facemask for maxillary protraction is to increase the efficiency of an appliance that needs patient participation, to achieve better results in a shorter period of time, to minimize unnecessary dentoalveolar effects, and to achieve more skeletal effects. Increasing the skeletal effect can reduce post-treatment relapse.7, 8, 9 Face masks with the rapid maxillary expansion (RME) appliance, skeletal anchorage, and Alternate Rapid Maxillary Expansion and Constriction (Alt-Ramec) protocol are used to increase the skeletal efficacy in the procedure.
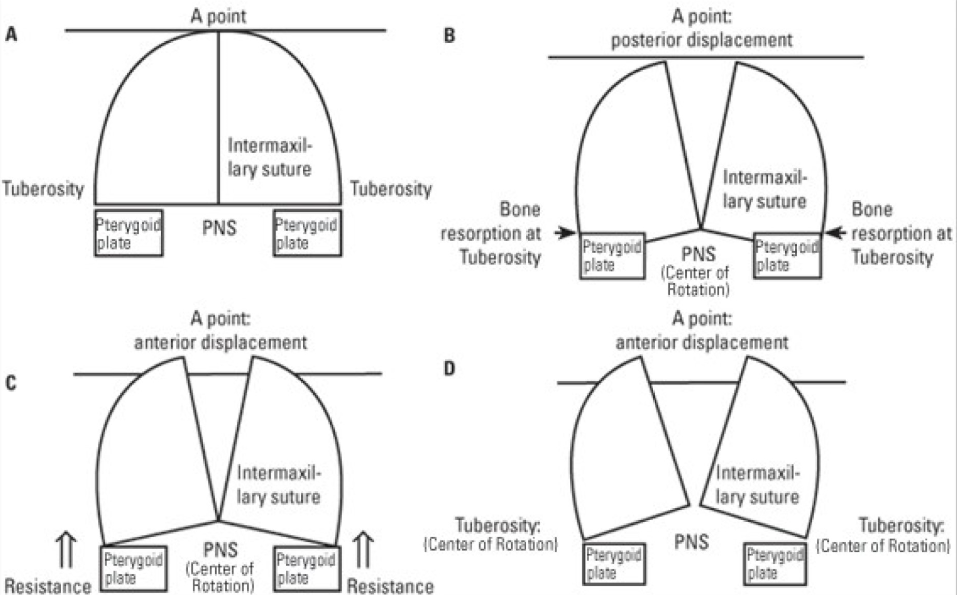
Figure 1
Alt-Ramec. A) Maxilla before expansion.; B): Posterior displacement of maxilla after RME.; C): Anterior displacement of maxilla by hyrax expander using Alt-Ramec protocol.; D): Anterior displacement of maxilla by double hinged expander using Alt-Ramec protocol.

Alt-Ramec
The Alt-RAMEC protocol was introduced by Liou in 2005. 10 It was created to open the circumaxillary sutures without the drawbacks of maxillary overexpansion. In contrast to traditional RME, its implementation technique is to increase the frequency of rapid maxillary expansion by alternating rapid expansion and constriction for many times. Its logic is analogous to that of basic tooth extraction, in which we continuously rock the tooth buccally and lingually until it is "disarticulated" out of the alveolar socket.11
Sutural expansion or protraction osteogenesis is the process by which new bone is formed by mechanically stretching the craniofacial sutures. The biological response to the mechanical traction created by Alt-Ramec protocol, includes widening of the sutures, changes in the fiber bundle orientation, increase in the number of osteoblasts and the deposition of osteoid on both sutural bone surfaces. Rapid maxillary expansion is an example of sutural expansion osteogenesis. Maxillary protraction is also an example of sutural protraction osteogenesis. Both of these treatment modalities involve separation of all the circummaxillary sutures with concomitant osteogenic activity histologically. The main premise of this treatment is that the maxillary expansion “disarticulates” the circummaxillary sutures so that the facemask traction becomes more productive.
In Alt-Ramec protocol, the maxilla is expanded at the rate of 1 mm/day for first week by opening the screw and then this screw is closed at rate of 1 mm/day in second week. In the remaining weeks the screw is turned on for one week and closed for one week. This can be continued for 7-9 weeks. Following completion of this protocol, protraction force is applied to move maxilla forward. This protraction force is usually applied using reverse pull headgear.11
Liou et al. explained various changes that took place in maxillae with RME and Alt-RAMEC in the introductory article. In Rapid maxillary expansion, the center of rotation of maxillae is located on posterior nasal spine. Depending on the level of resorption in the maxilla, the tuber maxillae shift forward and backward while the A point remains in the same place. In Alt-Ramec protocol also the center of rotation of the maxillae is located at the PNS, and the tuber maxillae move forward more without any resorption in the maxilla. This is the reason why there is enhance forward movement of maxilla in Alt-Ramec then RME. (Figure 1) 11
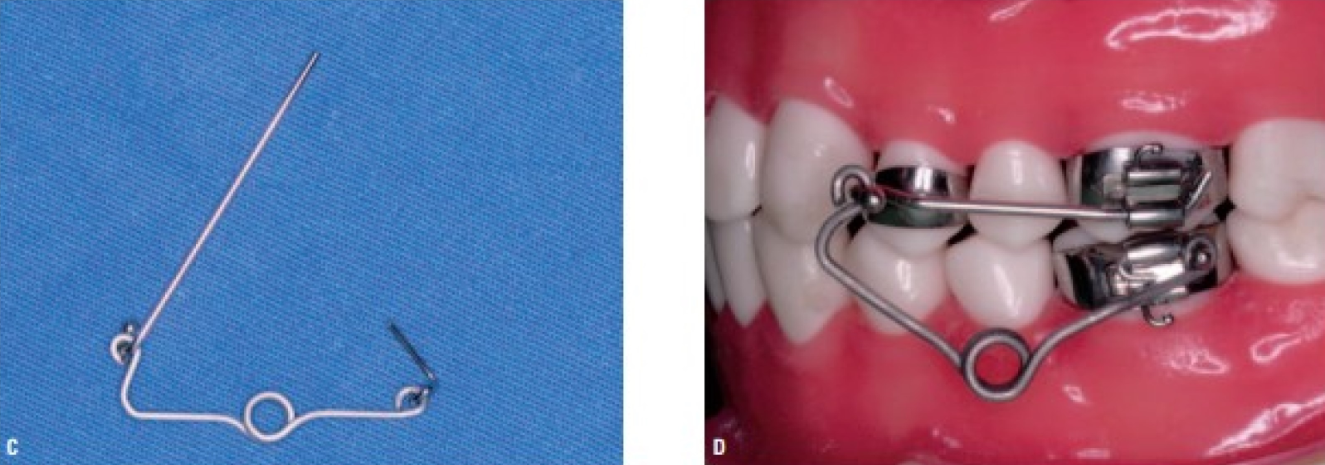
Screw type used in Alt-Ramec
In the previous years, a double-hinged hyrax screw as developed by Liou was used.10 In the recent years, this protocol was successfully applied with standard hyrax screws. No study has investigated the effect of screw type on protocol or craniofacial and dentoalveolar construction. (Figure 2, Figure 3)
Different protocols for Alt-Ramec
The most commonly used protocols for Alt-Ramec are 7 weeks and 9 weeks protocol. There have been few studies that compare Alt-RAMEC protocols. In the study done by Celikoglu et al. in which skeletal and dental changes after 5 weeks and 9 weeks protocol were compared, the results show that effects of the two protocols are similar.12
Comparison of RME and Alt-Ramec
Use of facemask after RME and after the application of Alt-Ramec protocol and the changes associated with these have been compared in many studies.
Liou EJ and Tsai WC 10: In this study, patient with unilateral cleft lip and palate were divided into two groups. First group was treated with RME applied using a hyrax screw for 1 week. Second group was treated with Alt-ramec protocol applied for nine weeks. Intraoral maxillary protraction springs were used for maxillary advancement in both the groups for 6 months. The results suggested that more protraction was obtained in At-Ramec group (point A moved by 5.8±2.3 mm) than RME group (point A moved by 2.6±1.5 mm).
Do-delatour et al. 13: This study compared the difference in the amount of maxillary protraction when carried out with either 7 weeks of Alt-RAMEC or 1 week of rapid maxillary expansion. The pilot study consisted of eighteen consecutively treated patients with either the Alt-RAMEC protocol or rapid maxillary expansion alone. Their results indicated that Alt-RAMEC alone does not increase the amount of forward movement of the maxilla and that other factors such as patient age, the duration of facemask worn, and the treatment duration need to be considered. The study also stated compliance was less in Alt-ramec group as compared to RME group.
Viera et al.14: This study was conducted in 20 patients with unilateral cleft lip and palate. The reports concluded that the effects of RME and Alt-Ramec are similar.
Isci et al.15: In this study, the dentofacial effects were evaluated for 1-week rapid palatal expansion versus activation deactivation protocols with protraction headgear. The RME group were underwent expansion the for 1 week while the activation deactivation group were instructed to expand and contract weekly for 4 weeks. Protraction headgear was used by both the groups for 12 months. The results indicate that the anterior movement of point A in the activation deactivation group was approximately twice that for the expansion only group. The backward movement of the mandible showed no significance between both groups and neither did the anterior facial height increase. This they concluded that the anterior movement of point A demonstrated that the activation deactivation protocol positively affects maxillary protraction.
Wilmes et al.16: This study reported that the maxillary protraction is better using Alt-Ramec protocol then conventional RME therapy.
Masucci et al.17: The results of this study shows that the SNA angle, ANB angle and Wit’s value increased significantly more in Alt-Ramec then RME.
Liu et al.18: When 7 week Alt-Ramec protocol was compared with RME, it was found that the Alt-Ramec protocol was more successful for maxillary protraction and yielded less posterior rotation of mandible.
Other articles related to Alt-Ramec
1. Wang et al.6 did a study to assess the amount of circummaxillary opening in the Alt-RAMEC protocol and for this he harvested the craniofacial skeletons of 12 inbred cats. They were divided into 2 groups. Maxillary expansion for 1 week was performed in one group while the Alt-RAMEC protocol for 5 weeks was performed in the other group. Histological analysis of the circummaxillary sutures indicated that Alt-RAMEC opens both the sagittally and coronally running circumaxillary sutures quantitatively more than conventional RME. It was also concluded that the opening of the coronally running circumaxillary sutures required Alt-Ramec for more than 5 weeks.
2. A systematic review was done by Pithon et al.19 to assess the effectiveness of early treatment of Class III malocclusion using Alt-Ramec protocol and facemask. It was concluded that Alt-Ramec is better than RME. It was also concluded that studies regarding relapse, recurrence and long term outcomes are required.
3. A systematic review and meta-analysis was conducted for comparative assessment of the dentoalveolar, skeletal and soft tissue effectiveness of Alt-RAMEC/PFM therapy and RME/PFM therapy.20 It was concluded that the skeletal effects contributing towards enhancement of profile was better in Alt-Ramec than RME. Dentoalveolar changes measured in this review did not show much difference between two protocols and data was insufficient for assessing the soft tissue changes.
4. Yilmaz BS, Kucukkeles N21 evaluated the effect of Alt-Ramec on skeletal structures, soft tissue, and airway. A double-hinged expansion screw was used in 20 patients with Class III skeletal malocclusion characterized by maxillary retrognathia. The results showed that Point A moved slightly forward and downward. Along with expansion of maxilla, the forces also caused separation of the nasal bone, the zygomaticomaxillary and zygomaticotemporal sutures. The soft tissue nasal width increased significantly. An increase in airway volume of the anterior nasal compartment and the nasal cavity was seen.
5. A retrospective study was conducted by Narayan H. Gandedkar and Eric Jein-Wein Liou22 to evaluate effects of Alt-Ramec on alveolar bone surrounding the anchor teeth. Conclusions of this study stated that the buccal alveolar bone thickness of anchor teeth reduced after expansion. Long term studies are needed in this area.
Conclusion
Based on this literature review, it can be concluded that use of Alt-Ramec protocol before maxillary protraction can be effective method for early treatment of Class III malocclusion. The skeletal and soft tissue changes seen with Alt-Ramec are better than traditional RME. Alt-Ramec has a problematic effect on alveolus of anchor teeth used for the expander but the changes are within the range of the original thickness of the alveolus so destructive changes are not seen. Further, studies pertaining to long term effects of the At-Ramec are required.