- Visibility 86 Views
- Downloads 7 Downloads
- DOI 10.18231/j.jsas.2021.026
-
CrossMark

An effective and simple method for treatment of tongue thrusting in adult patient- A case report
Introduction
The tongue is essential for several bodily functions, including swallowing, breathing, speaking, and chewing. Deglutition or swallowing is the act of moving food from the mouth to the stomach via the pharynx and oesophagus. Development of swallowing begins about 10-12 weeks after gestation. Full swallowing and suckling is established by 32-36 weeks of intra-uterine life.[1] Infantile swallow is characterized by active contractions of lip musculature and tip of the tongue is placed between the gum pads and the swallow is directed by the interplay of the tongue and the lips. Mature swallows develop between the ages of 4-5 years. Maturation of the swallow pattern occurs with the introduction of semisolid foods into the diet and the eruption of deciduous molars. It is distinguished by the relaxation of the lips, the positioning of the tongue behind the maxillary incisors, and the elevation of the jaw until the posterior teeth make contact.[2] A tongue thrusting habit occurs when the tongue makes contact with any teeth anterior to the molars during swallowing. Tongue thrust is an oral behaviour pattern associated with the preservation of an infantile swallow pattern throughout infancy and adolescence. Forward tongue posture and tongue thrusting during swallowing are said to be the most common signs of tongue thrusting, as are hyperactive mentalis and orbicularis oris buccinator hyperactivity, and swallowing without the normal momentary tooth contact.[3], [4] While anterior location, excessive of the tongue has been associated with open-bite, other theories suggest that tongue pushing behaviour may be a consequence of an open-bite that, in fact, may enable an otherwise nonexistent oral seal.[5], [6], [7] Tongue thrust has been associated to posterior crossbite, open bite, and excess overjet in terms of malocclusion.[8] Treatment for tongue thrust differs according to the cause of the related issues. Habit breaking appliance becomes tedious to use for adult patients. This article shows a method that can be effectively used for correction of tongue thrusting in adults.
Case history
A 19-year-old female patient reported to the department with a chief complaint of forwardly placed front teeth. Patient does not give any significant family history, medical history, dental history. Patient gave history of tongue thrusting habit. There were no findings on her fingers.



|
Measurement |
Mean |
Pre RX |
|---|---|---|
|
Skeletal |
||
|
SNA |
82o |
84o |
|
SNM |
80o |
80o |
|
ANB |
2o |
4o |
|
Saddle angle |
123+5o |
125o |
|
Gonial angle |
142+5o |
139o |
|
Convexity at pt. A |
2+2 mm |
0mm |
|
Facial Axis |
90+3o |
93o |
|
Inferences-class II Skeletal Pattern |
||
|
Growth Pattern |
||
|
Go-Gn to Sn |
32o |
26o |
|
FMA |
25o |
22o |
|
Mandibular plane angle |
26+4.5o |
17o |
|
Jaraback ratio |
62-65% |
70% |
|
Inferences-Horizontal growth pattern |
|
Dental |
||
|
U1-NA angle |
22o |
30o |
|
U1-NAmm |
4mm |
7mm |
|
L1-NB angle |
25o |
38o |
|
U1-NB mm |
4mm |
8mm |
|
IMPA |
90o |
113o |
|
Inferences-Proclined maxillary and mandibular incisors |
||
|
Soft tissue |
||
|
S line |
||
|
Upper lip |
0mm |
5mm |
|
Lower lip |
0mm |
5mm |
|
H line angle |
7-15o |
20o |
|
Upper lip strain |
2mm |
4mm |
|
Facial angle |
90+3o8 |
89o |
|
Inferences-Protrusive upper and lower lips, increased lip strain |
On extra oral examination patient was diagnosed with a mesoprosopic facial form, potentially incompetent lips and convex profile. Smile arc is straight. Intra-oral examination shows spacing in maxillary and mandibular anteriors, class I incisor relationship, Class I canine and Class I molar relation on right side and end on canine and molar relation on left side.
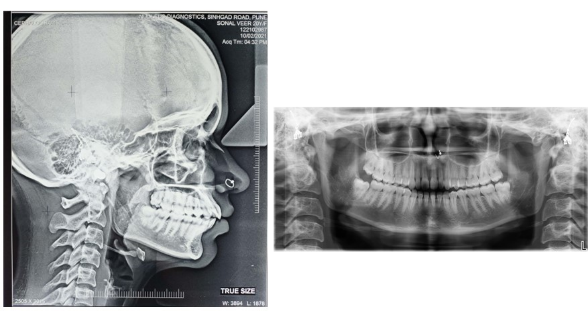
Orthopantomogram examination shows normal condylar morphology bilaterally. All third molars are present and roots are still forming. The level of alveolar bone was normal years. On cephalometric examination, patient has Class II skeletal pattern, proclined maxillary and mandibular incisors, protrusive upper and lower lips, increased lip strain, horizontal growth pattern. Diagnosis- A 23 years old female patient is diagnosed with Class II skeletal pattern, average to horizontal growth pattern, Class I molar relation on left side, Class II molar relation on right side, class I canine relation on left side, Class II canine relation on right side Class I canine relation left side, class II division 1 incisor relation, proclined upper and lower incisors, protrusive upper and lower lips, increased lip strain.
Treatment objectives
The main objective of the treatment was to eliminate the tongue thrusting habit which is aetiology of malocclusion here. The other treatment objectives were to improve the profile, lip competency, smile, to achieve normal overjet, overbite and correct proclination of maxillary and mandibular anteriors.
Treatment plan
Correction of tongue thrusting should be done along with commencement of fixed orthodontic treatment for correction of this malocclusion. Banding of all first molars should be done. A 0.022’’ slot preadjusted Edgewise appliance brackets with MBT prescription will be used in maxillary and mandibular arch. Extraction of all first premolars is planned after initial leveling and alignment with round NiTi wires, following sequence A of MBT. Use of 0.019/0.025” rectangular NiTi followed by 0.019/0.025” rectangular stainless steel wires for retraction and closure of spaces. Finishing and detailing will be done. Lingual bonded retainer will be given in both arches.
Treatment mechanics
Fixed orthodontic treatment was started according to the treatment plan. For tongue thrusting correction, spikes made of composite on the palatal side of upper central incisors were used so that patient does not thrust tongue between the teeth. With help of floss, an elastic module placed in between the central incisors. This will condition the patient to place tip of the tongue on palate behind the maxillary central incisors which is the normal tongue position.
Discussion
Comprehensive evaluation and treatment planning are required for successful orthodontic therapy.[9] Dental malocclusion can be caused by a variety of environmental variables, including oral habits. The severity of a malocclusion caused by oral habits is determined by the frequency, duration, and intensity of the habit. These behaviours interfere with muscle balance and bone development, resulting in alterations to the dental arch and occlusal features.[10], [11] Hence, it is important to diagnose habits and correct them at appropriate time to avoid these harmful effects.
Tongue-thrust swallowing is described as the forward positioning of the tongue tip between the incisors during deglutition. Tongue thrusting is a behaviour in which the tongue makes contact with any teeth anterior to the molars when swallowing.[12] The most essential factor for correcting the tongue thrusting behaviour is to change the resting posture of the tongue. Orthodontic spikes, prongs, or other tongue reminders, which correct the tongue rest posture and swallow, may be used to treat tongue thrust. The method used in this article is effective for redirecting tongue position with minimal discomfort to patient.
Conclusion
Abnormal tongue position in the context of an anterior open bite must be evaluated and corrected with care. Before using habit-breaking appliances, it is advised to begin with the least intrusive approaches, such as therapy and counselling. Correction of tongue thrusting is important for avoiding malocclusions it may cause. Redirecting tongue position with method used in this case report is effective in correcting tongue thrusting in adults.
Source of Funding
None.
Conflict of Interest
None.
References
- J L Miller, B C Sonies, C Macedonia. Emergence of oropharyngeal, laryngeal and swallowing activity in the developing fetal upper aerodigestive tract: an ultrasound evaluation. Early Hum Dev 2003. [Google Scholar] [Crossref]
- C L Peng, P G J Brinkmann. Comparison of tongue functions between mature and tongue-thrust swallowing-an ultrasound investigation. Am J Orthod Dentofac Orthop 2004. [Google Scholar] [Crossref]
- M L Hanson, L W Barnard, J L Case. Tongue-thrust in preschool children. Am J Orthod 1969. [Google Scholar] [Crossref]
- C L Peng, P G J Brinkmann, N Yoshida, H H Chou, C T Lin. Comparison of tongue functions between mature and tongue-thrust swallowing: An ultrasound investigation. Am J Orthod Dentofacial Orthop 2004. [Google Scholar] [Crossref]
- A A Lowe, W D Johnston. Tongue and jaw muscle activity in response to mandibular rotations in a sample of normal and anterior open-bite subjects. Am J Orthod 1979. [Google Scholar] [Crossref]
- T R Wallen. Vertically directed forces and malocclusion: A new approach. J Dent Res 1974. [Google Scholar] [Crossref]
- A S Cayley, A P Tindall, W J Sampson, A R Butcher. Electropalatographic and cephalometric assessment of tongue function in open bite and non-open bite subjects. Aust Orthod J 2000. [Google Scholar]
- J D Subtelny. Examination of current philosophies associated with swallowing behavior. Am J Orthod 1965. [Google Scholar]
- T Sinem, S Biren, C Ceylanoglu. Tongue Pressure Changes Before, During and After Crib Appliance Therapy. Angle Orthod 2010. [Google Scholar] [Crossref]
- E Larsson. Dummy- and finger-sucking habits with special attention to their significance for facial growth and occlusion. 4. Effect on facial growth and occlusion. Svensk Tandlakare Tidskr Swed Dent. Swed Dent J 1972. [Google Scholar]
- P Frazao, P C Narvai. Socio-environmental factors associated with dental occlusion in adolescents. Am J Orthod Dentofacial Orthop 2006. [Google Scholar] [Crossref]
- M L Falk. Neuromuscular facilitation for the control of tongue thrust swallowing.. Am J Orthod 1987. [Google Scholar] [Crossref]