
Introduction
Sigmoid volvulus is a condition in which torsion of the sigmoid colon around its mesenteric axis, which leads to acute large bowel obstruction, which not treated timely and properly, leads to life-threatening and morbid complications, like bowel ischemia, gangrene and perforation and also death.1, 2 so required early and correct diagnosis which is very essential for proper and timely treatment, which is required to correcting abnormal pathophysiological changes and restoring intestinal changes which is caused by the volvulus. Elderly, hospitalized patients and neurogenic disorders peoples are mainly affected. Emergency surgery is mainly done for those peoples who present with diffuse peritonitis, intestinal perforation or ischemic necrosis.3, 4 Colonoscopy used to evaluation of colonic mucosa [presence or absence of signs of ischemia.5, 6
The cause of SV is not known clearly. Main risk factors are long congenital sigmoid with a short mesenteric base, chronic constipation, high fibre diet, acquisitive mega colon, uses of anticholinergic drugs, sedatives and anti-Parkinson agents.7 Rotation of bowel always occurs in an anticlockwise and 180 degrees for complete rotation.8 SV is a very good example of closed loop obstruction. If the ileo-caecal valve is competent, a double closed loop obstruction developed and this result with huge distention of bowel.9, 10
Clinical features are abdominal pain, constipation and abdominal distention. elderly peoples who consuming psychotropic medications, pain is not common features, such patients mainly significant abdominal distention.11 diagnosis made by abdominal X-ray, enema, sigmoidoscopy, CT- scan and blood test.12, 13, 14, 15, 16
Materials and Methods
This is a prospective cohort study of 24 patients presented with the features of SV to govt. medical college Shahdol [tribal area of central India] from June 2022 to December 2022. We studied the causes of high incidence of SV, clinical features, management, complication and outcomes.
All suspected cases presented to casualty or outpatient, included in this study. Patients who present with other surgical emergencies and bowel perforation were excluded.
In data we included- age, sex, residency, socio-economic status, diet pattern, abuse, comorbidity, past history, clinical presentation, diagnostic and therapeutic measures, post-operative complications and outcomes were recorded. All data were recorded with frequency and percentage and presented in frequency tables.
Observation and Results
In our study, 24 patients presented with the clinical features of SV.
There were 21 (87.5%) male and 3 (12.5%) female patients, with the male to female ratio was 7:1.
The age distribution ranged from 30-70 years. The highest incidence was in the 50-70 years age group, in which 16 patients (66.6%).
Most patients are coming from rural area 22 [91.6%] with low socioeconomic status.
Most patients have pure vegetarian 18 [75%] consume high fibre rich diet.
Most commonly abused material ganja 20 [80%], alcohol 18 [75%], and tobacco 18 [75%] peoples.
Most common comorbidity is hypertension 14 [58.3%], hypertension with diabetes 10 [41.6%], diabetes 8 [33.3%], anaemia 7 [29.1%], hepatitis 4 [16.6%] and tuberculosis 2 [8.33%].
19 patients (79.1%) gave history of chronic constipation, 12 patients [50%] consumes high fibre diet, 3 patients (12.5%) were hospitalised with neuropsychiatric disorder, 2 patients [8.3%] have bed ridden due to previous surgery.
Table 1
Demographic factors
In our study, the main presenting symptoms were constipation and abdominal distension 23 patients (95.8%) followed by abdominal pain 21 [87.5%] and vomiting 22 (41.6%) patients. Main signs are tenderness 87.5%, tachycardia 83.3%, icterus 41.6%, respiratory distress and oliguria 12.5% cases.
Table 2
Clinical sign and symptoms
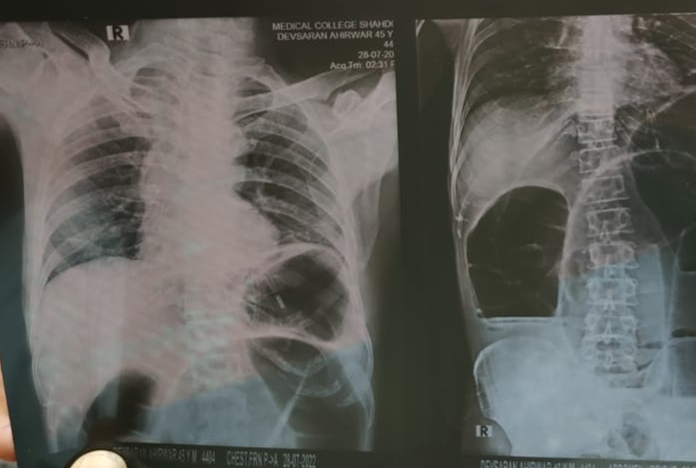
Investigated by plain abdominal X-ray and blood investigations done in all patients. Which showed characteristic features of sigmoid volvulus in 18 patients (75%), like- omega sign of the dilated colon [apex of the loop under the left hemidiaphragm and the convexity of the loop points towards the right upper quadrant], 3 (12.5%) showed distended ileal loops in a distended sigmoid colon and 3 patient (12.5%) showed free air under left hemi diaphragm.
On blood investigations, 20 patients (83.3%) had leucocytosis [16 of them have a WBC count >16000

All patients who were suspected clinically that, have an underlying strangulation, doing emergency exploratory laparotomy. 6 cases (25%) have intraoperatively found gangrenous bowel found. No patient managed by nonoperative management. The majority of these cases were managed by sigmoidectomy with colostomy/ileostomy in patients who had found gangrenous sigmoid colon or a sigmoid colon with questionable viability intraoperatively, after operative detorsion (17 patients, 70.83%).

In our study Paul-Mikulicz procedure was done in only 1 patient [4.1%]. New surgical modification technique Sigmoidectomy and colorectal anastomosis bypassing flatus tube was done in 6 patients (25%) and thus bypassing the stoma formation and future stoma closure.
Table 3
Treatment and complications
Most common post-operative complications are vomiting [33.3%], paralytic ileus [25%], anastomotic leak and obstruction [16.66%]. Majority of patients discharged [87.5%] and 12.5% patients died.
Results and Discussion
Osime U et al done a prospective cohort study of 25 patients, in patient with features of strangulated sigmoid colon volvulus. This study done in Al-Karama Teaching Hospital (surgical casualty) from March 2014 to March 2018. In this study 18 patients (72%) were males and 7 patients (28%) were females. The age ranged from 20-70 years. The main predisposing/risk factor were chronic constipation, laxative dependency and high fibre diet. The most common presenting symptoms and signs were absolute constipation, abdominal distension, tenderness, tachycardia and fever.17
In our study 21 patients (87.5%) were males and 3 patients (12.5%) were females. The age of the patients ranged from 30-80 years most of them ranged between 50-70 years. The main risk factor was1 old age,2 male sex,11 rural residency,18 low socioeconomic status,3 pure vegetarian diet,4 abuse [mc- alcohol],19 chronic constipation,20 chronic pain killer user5 associated comorbidity [mc- hypertension[10] high fibre diet has more chances of this.
In our study the most common presenting symptoms were absolute constipation and generalized abdominal distension followed by abdominal pain. Most common signs were tenderness followed by tachycardia and then fever. All the patients were investigated by clinical symptoms, plain abdominal erect X-ray and blood investigations
Friedman et al, studied that, as sigmoid volvulus is a disease which is associated with high morbidity and mortality and high recurrence following non-operative decompression or non-operative line of management, therefore in all patient’s definitive surgery is required.21 Similarly Mokoena TR et al, studied in 90 cases of sigmoid volvulus and advocate that resection in all patients.22 similarly Baker DM et al, saying that, a colostomy rather than primary anastomosis is indicated if emergency surgery done.23
In our study vomiting most common postoperative complication followed paralytic ileus. Among the patients, 6 had distended gangrenous SV, 15 patients were discovered to have distended non-gangrenous and the 3 patients had a perforated gangrenous sigmoid colon volvulus. Mostly treated by sigmoidectomy with stoma followed by resection with colorectal anastomosis bypassing flatus tube.
Bagarani M et al, also saying that, resection with primary anastomosis in patients with viable colon and colostomy in patients with strangulated colon, the treatment of choice in sigmoid colon volvulus.24 the morbidity and mortality rates were highest in strangulation patients (16%) and the latter was (4%). There are nearly similar results are found to other studies:
Mokoena et al, also reported a (20%) morbidity rate and (12%) mortality rate, there are mostly of which was in the emergency operating group.22 similarly Osime U, studied that a (7.9%) mortality rate after resection of strangulated sigmoid colon volvulus.17
In our study 12.5% patients’ death and most of the patients discharged.
Conclusion
SV is more common in males. Middle-old age individuals found most affected group.in the study Majority of patients with SV was [1] old age, [2] male sex, [3] rural residency, [4] low socioeconomic status, [5] pure vegetarian diet, [6] abuse [mc- alcohol], [7] chronic constipation, [8] chronic pain killer user [9] associated comorbidity [mc- hypertension] [10] high fibre diet. The main presenting symptoms and signs of patients are abdominal distension and tenderness, tachycardia and fever with abdominal distension and absolute constipation. All the patients were investigated by clinical symptoms, plain abdominal erect X-ray and blood investigations. Vomiting most common postoperative complication followed paralytic ileus. Among the patients, 6 had distended gangrenous SV, 15 patients were discovered to have distended non-gangrenous and the 3 patients had a perforated gangrenous sigmoid colon volvulus. Mostly treated by sigmoidectomy with stoma followed by resection with colorectal anastomosis bypassing flatus tube. Majority of patients discharged, only 3 [12.8%] patient died.