- Visibility 49 Views
- Downloads 32 Downloads
- DOI 10.18231/j.jsas.2023.005
-
CrossMark

Role of arthroscopic knee lavage supplemented with intra-articular methy l prednisolone in osteoarthritis of knees
Introduction
Osteoarthritis also known osteoarthrosis degenerative joint disease and degenerative arthritis is a heterogeneous group of disorders that results in articular cartilage degeneration. It characterized by disturbance of smooth property of cartilage resulting in formation of subchondral cysts and marginal osteophytes. These processes continue until the full thickness of cartilage is lost and bone is left exposed. It is not a single disease entity but a final common pattern of joint failure.
Keuttner and Goldberg described osteoarthritis as a group of overlapping diseases which may have different etiologies, but with similar biological, morphological and clinical outcomes. The disease process not only affects the articular cartilage but involves the entire joint including the subchondral bone, ligament, capsule, synovial membrane and periarticular muscles, ultimately the articular cartilage degenerates with fibrillation, fissures, ulceration, and full thickness of the joint surface gets involved. The most commonly involved joint is the knee reported prevalence of osteoarthritis in rural India is accounting for thirty percent of all rheumatological problems.
Various risk factors as enumerated by Hochberg include; age, female gender, race ,quadriceps weakness, obesity, genetic factors, joint trauma, repetitive stress and joint overload, congenital disorders, prior inflammatory disorder, metabolic/ endocrine disorders.[1]
Problems to the patient
Pain, starts insidiously and increases slowly over months and years. It is aggravated by exertion and relieved by rest. In late stage the patient may have pain in bed at night.
Stiffness characteristically occurs after period of inactivity.
Swelling may be intermittent (suggesting an effusion) or continues with capsular thickening and osteophytes.
Deformity results from capsular contracture or joint instability.
Kellgren and Lawrence graded osteoarthritis into five grades based on radiological findings[2]
Grade 0 Normal findings
Grade 1 questionable presence of joint space narrowing or both
Grade 2 definite presence of osteophytes with possible joint space narrowing or mild joint space narrowing
Grade 3 definite moderate joint space narrowing at least fifty percent Osteophytes usually present
Grade 4 severe joint space narrowing
Grading the joint pain
Pain is a subjective symptom and its’ varies from person to person and can never be quantified exactly. However, from time to time an attempt has been made to grade the joint pain and different methods include;
Likert scale: a five point scale depending upon the patients’ own perception of pain
None, mild, moderate, severe, very severe.
Visual analogue scale; In VAS a 100 mm line free of marking is commonly used and patient is asked to mark the amount of pain at each visit.
Treatment modalities
Treatment of osteoarthritis currently aims in reducing the pain and stiffness and at the most slowing of disease process.
Pharmacological treatment includes Acetaminophen, NSAIDS, Salicylates, selective COX2 inhibitors, topical agents, intra-articular, glucosamine, and chodroitin sulphate.
Non – Pharmacological and Non- surgical treatment includes physiotherapy, decreasing load on the joint through life style modifications i.e. weight loss, rest , movement of joint to full range of motion several times a day to prevent capsular contracture, traction is used during acute inflammatory phase, warm dry fomentation.
Surgical treatment includes arthroscopic lavage, joint debridement, cartilage grafting, realignment osteotomy and arthroplasty.
Knee lavage and local corticosteroids in osteoarthritis of the knee
Although osteoarthritis is classically thought as a degenerative process there is always mild inflammatory process, which further acts as mediator of cartilage damage. Intra-articular debris especially cartilage are found in the joint which cause mechanical irritation and degenerative enzymes like collagenases, elastases, and cytokines cause chemical irritation and produce synovitis.
Thus a vicious cycle is set in. Along with these factors there are intra-articular adhesion and capsule fibrosis. Joint lavage in osteoarthritis of knees removes the debris, disrupts the adhesions and fibrosis. It also removes the degenerative enzymes and chemicals and significantly decreases the stiffness and pain and increases the joint motion. Arthroscopic joint lavage is a simple procedure under local anesthesia without any restrictions in day today activities and is highly cost effective.
It appears to be an excellent economical treatment modality in a developing country like India. Keeping these things in mind we conducted a prospective study in the OrthopedicDepartment in the government medical college Amritsar.
Aims and Objectives
The present study is aimed at to achieve the objective of evaluating intra-articular methyl prednisolone 80 mg in osteoarthritis of knee joint with reference to relief of pain.
Materials and Methods
Patients
Hundred consecutive knees in patients of either sex having symptomatic osteoarthritis of the knee reporting to the Orthopedics department of the government medical college amritsar. Were included in the study. Detailed history and clinical examination was performed as per performa attached.
Exclusion criteria
Patients with raised fasting blood glucose levels, having generalized or local signs of infection were not included in the study. Patients with hypersensitivity to corticoids, osteochondritis dessicans, joint replacement and bacterial endocarditis were also excluded from the study. Uncontrolled bleeding and clotting disorders were not included in this study.
Treatment protocol
Every patient was subjected to arthroscopic knee lavage with 3000 ml of ringer lactate solution under fully aseptic conditions in operation theatre.10 ml, 2 percent lignocaine was used as a local anesthetic. at the end of procedure eighty mg of methyl prednisolone was injected through a spinal needle inserted in the suprapatellar pouch. Patient was sent home with instruction for restricted activities for 24 hours only. Post operatively patients were mild analgesic and an antibiotic for 7 days .after one week bandage was removed and band-aid applied for other five days. Patients were called at 1 month, 3 months, and 6 months follow-up for evaluation.
Procedure
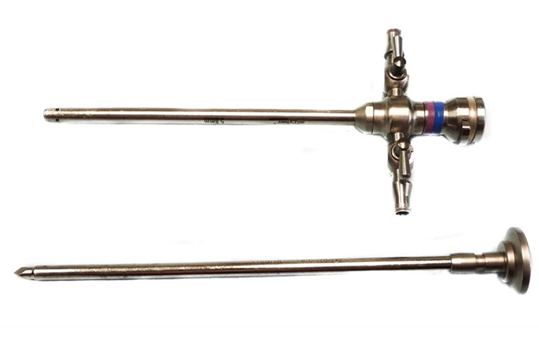
In the operation theatre after thoroughly cleaning the knee, the area was painted with povidone iodine solution and draped with sterile sheets. A point was marked one finger breadth below the tibial plateau, outside the lateral border of patellar tendon while the knee was flexed at 45 degrees. 10 ml, 2% lignocaine was infiltrated through this point into the knee and in the subcutaneous tissue. A stab incision was given with a number 11 blade with the knife handle making an angle of 45 degrees to the leg and the ground. The blade was pushed forwards, upwards, and medially. Three way arthroscopic cannula was inserted along with the blunt trocar (Figure 1) into the knee through the opening. During this procedure knee was brought into full extension. After stabilizing the patella with the palm of the other hand, trocar and cannula assembly will be swiped sideways few times to break the intra – articular adhesions and smoothen the undersurface of patella. The trocar was removed and the effusion was drained out. The tip of I.V. set was attached to the side opening of cannula and lock opened to run fluid into the joint. The main proximal opening of cannula was blocked with the thumb so to fill the joint. Once the joint was full of fluid as analysed by the bloating of supra patellar area, the side lock was closed and joint emptied with the gush by pressing and squeezing the supra patellar area with one hand and releasing the thumb block of arthroscopic cannula at the same time. This filling and emptying of the joint was repeated and 3000ml of ringer lactate was used. After the lavage an injection of 80 mg of methyl prednisolone was injected into the knee through a spinal needle attached to 10 ml syringe, admixed with xylocaine. The cannula locks were closed and the knee flexed and extended a couple of times to ensure the uniform distribution of the drug into the joint. Antiseptic dressing and a crepe bandage was given and the patient would walk out of the operating room.
Evaluation of the patients
On admission, X-rays for AP view of both the knees in standing position were taken and osteoarthritis was graded based on Kellgren and Lawrence grading. Before the surgery and at every follow up patients’ pain perception was evaluated as per subjective perception marked on the Visual Analogue Scale where the patient marked a dot on a 100 mm long. Pain score was presumed to be maximum at the start of the treatment.
Evaluation of results
Depending upon improvement in pain score as per VAS the results were graded as follows;
Excellent 90-100% improvement
Good 70-89% improvement
Fair 40-69% improvement
Poor less than 40% improvement
Results
We enrolled patients of osteoarthritis of knee joint (Grades 1 to 3 the Kellgren and Lawrence radiological grading) coming to the out – patient department of Government Medical College, Amritsar for the purpose of the study. 100 knees in 75 patients were subject to knee lavage with 3 litres of ringer lactate solution under local anesthesia supplemented with intra- articular injection methyl prednisolone of 80 mg. All the patients turned up for follow up at different intervals and observations were recorded as per Performa attached.
Age and sex distribution
Of the total 51 patients were females and 24 were males. Fifteen patients were in the age group of 40 to 49 years, out of 9 females in the group 5 had 1 knee and 4 had both the knees involved and 6 males in this age group had only 1 knee involved. Thirty four patients in the group of 50 to 59 years, out of 22 females in this age group. 10 had 1 knee and 12 had both the knees involved. Out of 12 males in this age group 9 had 1 knee and 3 had both the knees involved. Twenty six patients were in the age group of 60 years and above. Out of 20 females in this age group 16 had 1 knee and 4 had both the knee involved. Out of 6 in this age group 4 had 1 knee and 2 had both the knees involved. Total number of patients with unilateral involvement of knee joint was 50 (66.6%) and bilateral involvement 25 (33.37%)
Total number of female patients 51 (68%)
Duration of knee pain
Of the 100 OA knees 30% had pain of less than one year, 25 percent had pain between 1-2 years, 18 percent had pain of 2-3 years and 15 percent had pain between 3-4 years and 12 percent had pain more than 4 years. The average duration of knee pain was 2.57 years.
|
Duration of knee pain |
Number of knees in patients |
Percentage |
|
Less than one year |
30 |
30 % |
|
1-2 years |
25 |
25% |
|
2-3 years |
18 |
18% |
|
3-4 years |
15 |
15% |
|
More than 4 years |
12 |
12% |
Radiological grading of osteoarthritis knee
Out of 100 knee joints that completed the study 5 percent were grade one, 10 were in grade two, 55 were in grade 3, and 30 were grade 4 as per Kellgren and Lawrence radiological grading for OA of the knee joint.
|
Radiological grades |
Number of knees |
Percentage |
|
Grade 0 |
None |
- |
|
Grade 1 |
5 |
5 percent |
|
Grade 2 |
10 |
10 percent |
|
Grade 3 |
55 |
55 percent |
|
Grade 4 |
30 |
30 percent |
In the group 40 -49 years 2 knees had grade 1,4 had grade 2 , 12 had grade 3 and 1 had grade 4 osteoarthritis as per Kellgren and Lawrence radiological grades. In the age group of 50 to 60 years, 3 had grade 1, 6 had grade 2, 31 had grade 3, 9 had grade 4 osteoarthritis as per Kellgren and Lawrence radiological grades, and 60 years and above group had no case of grade 1 and grade 2 osteoarthritis, 12 cases of grade 3 and 20 cases of grade 4 osteoarthritis as per Kellgren and Lawrence radiological grades.
In our study after one month, grading of results was done. Out of 100 knees 37% showed excellent, 37% showed good, 23% showed fair and 3% showed poor results. Of the 37 knees showing excellent results 4 had grade 1 osteoarthritis, 7 had grade osteoarthritis, 26 had grade 3 osteoarthritis. Out of 37 knees showing good results 1 had grade 1, 3 had grade 2 , 20 had grade 3 and 13 had grade 4 osteoarthritis. Out of the 23 knees showing fair results, 9 had grade 3 osteoarthritis, 14 had grade 4 osteoarthritis. Out of 3 knees showing poor result, all had grade 4 osteoarthritis.
Results at 3 months
In our study after three months grading of results was done again. Out of 100 knees, 40% showed excellent, 30 % showed good, 27% showed fair and 3% showed poor results. Of the 40 knees showing excellent results, 3 had grade 1 osteoarthritis, 7 had grade 2 osteoarthritis, 30 had grade 3 osteoarthritis. Out of 30 knees showing good results, 2 had grade 1 osteoarthritis, 3 had grade 2 osteoarthritis, 20 had grade 3 osteoarthritis and 5 had grade 4 osteoarthritis as per Kellgren and Lawrence radiographic grading of osteoarthritis. Out of 27 knees showing fair results, 5 had grade 3 osteoarthritis, 22 had grade 4 osteoarthritis. Out of 3 knees showing poor results, all had grade 4 osteoarthritis.
Results at 6 months
In our study after six grading of results was finally done. Out of 100 knees, 37% showed excellent, 30%showed good results, 30% showed fair results, 3% percent showed poor results. Out of 37 knees showing excellent results, 3 were grade 1 osteoarthritis, 6 were grade 2 osteoarthritis, 28 were grade 3 osteoarthritis.
Analgesic requirements
At the start, out of the 75 patients included in this study,5 (6.6 percent) patients were taking on analgesic tablets, 20(26.6 percent) took 1 tablet daily, 30 (40 percent)2 tablets daily, 15 (20 percent) patients took 3 tablets daily, and 5 (6.6%) patients took more than three tablets daily.
However, at 6 months follow up 15 (20 percent) took no tablets, 35 (46.6 percent) took one tablet, 25 (33.3 percent) patients took 2 tablets daily.
Discussion
The age of patients in our study varied from a minimum of 40 years to a maximum of seventy-five years with an average of 58 years. In our series and most studies in literature there is a female predominance. The female predominance may be due to increased obesity among females, post menopausal bone changes, and frequent kneeling and squatting for religious and household activities in Indian females. It is also clear from our study that articular cartilage is strong enough to sustain cyclic loading before 40 years of age. The minimal cartilage changes occur are not sufficient to cause clinical problem. The duration of pain in our study was over one year in all patients and half of them had pain more than three years. The average duration was 2.57 years. Lack of knowledge about the available treatment and poverty are the main reasons for the patients’ long sufferings in India before landing up for proper treatment. Knee joint crepitus was present in 82 knees out of 100 knees. The main outcome measure recorded in our study was knee pain and recorded at one, three and six month intervals. At one month the results were excellent in 37 percent knees, while at three months were 40 percent, and 37 percent at six months.
Our study showed that at six months out of total of 55 knees with grade 3 osteoarthritis 87.2 percent showed excellent or good results.
To elucidate the relief reported after these procedures, some have suggested that the fluid circulated through the knee during arthroscopy removes painful detritus and inflammatory enzymes from the knee.[3], [4],[5] Others have proposed that the improvement is the result of the removal of articular cartilage flaps, torn meniscal fragments, hypertrophied synovium, and loose detritus.[5],[6]
Role of steroids in knee pain
By modulating the T cells and B cells, steroid hormones suppress inflammation. Intra-articular steroid (anti-inflammatory drug) therapy is a feasible treatment, as it directly attacks the afflicted joint, and has minimal systemic impact. The present recommendations of The European League against Rheumatism, The American College of Rheumatology, and the Osteoarthritis Research Society International all recommend intra-articular steroid injections for the treatment of hip OA. However, as the panel of The American College of Rheumatology has observed, research emphasizing on patients with symptomatic knee osteoarthritis is lacking.[7] Triamcinolone acetate and methylprednisolone are the two medications now utilized most frequently to treat knee osteoarthritis. Because it is less water soluble than methylprednisolone triamcinolone is a preferable option for diabetics worried about post-injection spikes in blood sugar.[8] It requires 3 weeks for triamcinolone acetonide to be completely absorbed by the joint, and it may be detected in plasma after 6 weeks, where it typically stays for only 2.5-4.3 days. Effective pain alleviation from triamcinolone acetonide with extended release lasts for more than 12 weeks.[9] Patients with osteoarthritis (OA) reported significant pain relief after receiving an intra-articular injection of sustained-release triamcinolone acetonide.[10] A prior study found that methylprednisolone acetate considerably reduced early pain in OA patients, with the greatest effect occurring 2 weeks after injection and lasting for 24 weeks.[11]
In early OA patients, intra-articular injection of corticosteroids provides considerable symptom relief (14). However, the benefits of the treatment wear off quickly, typically within six months.[12] Our study showed that when combined with knee lavage the effect lasts longer than six months. Within 6 weeks of receiving a local injection of corticosteroid, the majority of patients with OA experience improved function[13],[14] Therefore, joints with symptoms should not be administered with articular corticosteroids more than four times per year.[15]
Summary and Conclusions
Our study demonstrates that arthroscopic knee lavage supplemented with methyl prednisolone is effective in osteoarthritis of knees for a relief more than six months. Knee lavage is more effective in patients with grade 1 or 2 osteoarthritis. The treatment reduces the need for analgesics and hence reduces the side effects that patients may suffer as a result of NSAID intake. Hence, this form of treatment can be used as an alternative to NSAIDS. Because this procedure is performed under local anesthesia it offers an economical treatment in patients on high doses of NSAIDs and unwilling or medically unfit to undergo a knee replacement surgery.
Source of Funding
None.
Conflict of Interest
None.
References
- DT Felson. Osteoarthritis: new insights. Part 2: treatment approaches. Ann Intern Med 2000. [Google Scholar]
- MD Kohn, AA Sassoon, ND Fernando. Classifications in Brief: Kellgren-Lawrence Classification of Osteoarthritis. Clin Orthop Relat Res 2016. [Google Scholar]
- RW Chang, J Falconer, SD Stulberg. A randomized, controlled trial of arthroscopic surgery versus closed-needle joint lavage for patients with osteoarthritis of the knee. Arthritis Rheumatism 2023. [Google Scholar]
- DJ Ogilvie-Harris, CH Choi, Osteoarthritis, J. Grifka and D. J. Ogilvie-Harris. . Arthroscopic Management of Degenerative Joint Disease 2000. [Google Scholar]
- NF Sprague. Arthroscopic debridement for degenerative knee joint disease. Clin Orthop Relat Res 1981. [Google Scholar]
- MR Baumgaertner, WD Cannon, JM Vittori, ES Schmidt, RC Maurer. Arthroscopic debridement of the arthritic knee. Clin Orthop Relat Res 1990. [Google Scholar]
- R Zamborsky, L Danisovic. Surgical Techniques for Knee Cartilage Repair: An Updated Large-Scale Systematic Review and Network Meta-analysis of Randomized Controlled Trials. Arthroscopy 2020. [Google Scholar]
- LA Wilson, J Liu, M Fiasconaro, J Poeran, BU Nwachukwu, SG Memtsoudis. Increased Use of Intra-Articular Steroid Injection to Treat Osteoarthritis is Associated With Chronic Opioid Dependence After Later Total Knee Arthroplasty But Not Total Hip Arthroplasty. J Arthroplasty 2020. [Google Scholar]
- SB Han, IW Seo, YS Shin. Intra-Articular Injections of Hyaluronic Acid or Steroids Associated With Better Outcomes Than Platelet-Rich Plasma, Adipose Mesenchymal Stromal Cells, or Placebo in Knee Osteoarthritis: A Network Meta-analysis. Arthroscopy 2021. [Google Scholar]
- AF Buyuk, E Kilinc, IY Camurcu, S Camur, H Ucpunar, A Kara. Compared Efficacy of Intra-Articular Injection of Methylprednisolone and Triamcinolone. Acta Ortop Bras 2017. [Google Scholar]
- N Maricar, MJ Parkes, MJ Callaghan, DT Felson, TW O’neill. Do Clinical Correlates of Knee Osteoarthritis Predict Outcome of Intraarticular Steroid Injections?. J Rheumatol 2020. [Google Scholar]
- G Habib, F Sakas, S Artul, F Khazin. The Effect of Periarticular Injection of Methylprednisolone Acetate in Patients with Primary Osteoarthritis of the Proximal Interphalangeal Joints: A Case Controlled Study. Pain Res Treat 2018. [Google Scholar] [Crossref]
- M Mclarnon, N Heron. Intra-articular platelet-rich plasma injections versus intra-articular corticosteroid injections for symptomatic management of knee osteoarthritis: systematic review and meta-analysis. BMC Musculoskelet Disord 2021. [Google Scholar]
- K Fredericksen, J Kiel. Bedside ultrasound-guided aspiration and corticosteroid injection of a baker’s cyst in a patient with osteoarthritis and recurrent knee pain. J Am Coll Emerg Physicians Open 2021. [Google Scholar] [Crossref]
- A Latourte, H Lellouche. Update on corticosteroid, hyaluronic acid and platelet-rich plasma injections in the management of osteoarthritis. Joint Bone Spine 2021. [Google Scholar]
- Introduction
- Problems to the patient
- Grading the joint pain
- Treatment modalities
- Knee lavage and local corticosteroids in osteoarthritis of the knee
- Aims and Objectives
- Materials and Methods
- Patients
- Exclusion criteria
- Treatment protocol
- Procedure
- Evaluation of the patients
- Evaluation of results
- Results
- Age and sex distribution
- Duration of knee pain
- Radiological grading of osteoarthritis knee
- Results at 3 months
- Results at 6 months
- Analgesic requirements
- Discussion
- Summary and Conclusions
- Source of Funding
- Conflict of Interest