
Introduction
Osteomyelitis is an inflammatory process of cancellous bone spreading to cortical bone, almost always involving mostly the mandible than maxilla. The mandibular angle region is an area of lowered resistance to external forces. A high percentage of mandibular fractures are located here. 1 Weakening the mandibular bone as a result of a decrease in its elasticity during advancing age may be a cause of the increased incidence of these fractures.2 Since the most common cause is odontogenic infections, the dentate part of mandible is generally involved and rarely does it extend to the condyle and coronoid processes.3 Even if involved, infections of the condyle or coronoid can either be of hematogenous origin, spread from adjacent structure or direct inoculation. Osteomyelitis is of two type; Primary chronic osteomyelitis is a non-suppurative chronic inflammation with no underlying cause. Whereas secondary osteomyelitis is usually suppurative and infective in origin developing secondary to acute symptoms,4 Most commonly from odontogenic infection, complications after tooth extraction, trauma periodontal infections, inadequate removal of necrotic bone,.5 According to Kim et al. 84.6% of osteomyelitis of the jaws is odontogenic in origin. The rarity of osteomyelitis of the coronoid process can be attributed it to being distant to tooth bearing areas of the jaw. Despite a distant site, osteomyelitis of condyle was most commonly odontogenic in origin with 8 out of 20 cases (40%) occurring either due to an infected 3rd molar, or infection following molar tooth extraction.6, 7
Case Presentation
A 45-year old male patient presented with a chief complaint of pain and swelling in the lower right back tooth region since 6 months. Patient presented with a swelling in the lower right back teeth region associated with occasional pain and restricted mouth opening. Patient visited a private clinic where extraction of 48 was done. After a week, he developed swelling with pain. Pain which was of intermittent in nature, dull aching, non-radiating, gradual in onset. Pain aggravated on mouth opening and mastication, not associated with relieving factors. There was no pus discharge/bleeding/mobile teeth/ fever/loss of weight etc. Previous medical history is non-contributory.
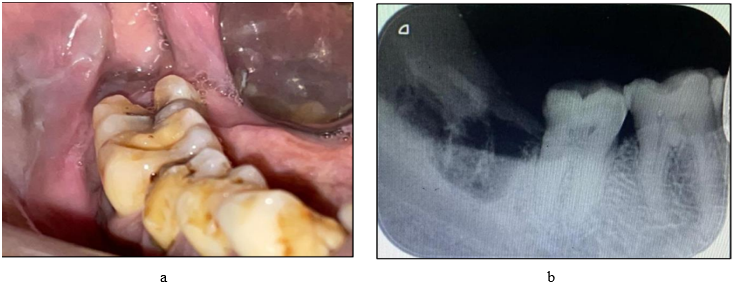


Figure 4
a: Vestibular incision given b: Fractured coronoid process removed c: Packed with amoxcillin powder d: Simple interrupted sutures given e: Excised specimen f: Follow up after 6 Months


On clinical examination there was a diffuse swelling present on right angle region of the mandible. Surrounding and surface skin was normal, On palpation there was mild tenderness in the near preauricular region. The swelling is associated with pain which is of intermittent in nature, dull aching, non-radiating, gradual in onset. Pain was aggravated by mouth opening and mastication, on examination of TMJ there was limited movement of TMJ nontender and no deviation on mouth opening. Submandibular lymph nodes were palpable and tender on the right side. A thorough oral examination revealed an absence for 48, with mild tenderness present posterior to 47 region. An OPG showed displaced coronoid process with loss of trabecular pattern and osteolytic changes along with extraction socket of 48. To know the extent of the lesion patient underwent a computed tomography scan (CT) revealed lytic changes with displaced right coronoid process. The patient was empirically placed on oral amoxicillin with clavulanic acid 625mg and metronidazole 400mg, Diclomol and Pan D for 5 days. Routine blood investigations were performed. All lab investigations were within normal limits. patient was subsequently operated under local anaesthesia for right coronoidectomy. Vestibular incision was taken from second molar on right side of mandible and extending till anterior border of external oblique ridge. Full thickness mucoperiosteum was reflected and the laterally displaced. Coronoid process was exposed and removed. sequestrectomy was performed around the socket of 48 thorough curettage and debridement followed by irrigation with povidone iodine was performed. Haemostasis achieved, Amoxicillin 1gm powder placed at the surgical site. Simple interrupted sutures were given along the incision. patient was advised to take oral medication for next 5 days. Histopathological examination revealed absence of osteocytes in the lacunae, absence of osteoblastic rimming. Bony trabeculae exhibited ragged margins with prominent reversal lines suggesting osteoclastic activity, marrow tissue consisted of inflammatory cell infiltrates overall findings suggested chronic osteomyelitis of coronoid process. On follow-up after 6 months and 1 year patient was free of symptoms with improved mouth opening and completely healed extraction socket of 48. No deviation of the jaw present and occlusion was satisfactory.
Discussion
The common postoperative complications of third molar extraction are alveolar osteitis, secondary infection, bleeding, and paraesthesia. On the other hand, major complications, such as mandibular fracture, severe haemorrhage, or iatrogenic displacement of the third molar teeth leading osteomyelitis are rarely reported.8 Among them, the incidence of mandibular fracture during or after a third molar extraction has been reported to be 0.0046% to 0.0049%.8 The patients aged between 42 to 50 years undergo demineralization secondary to osteoporosis which weakens the skeletal system. At the same time, narrowing of the periodontal ligament increases with age. In comparison to young patients, the tooth must be freed more extensively from the surrounding bone, and the jaw is further weakened.9 Older patients with a full dentition were considered to be a risk group Moreover, most fractures associated with the extraction of teeth develop osteomyelitis usually second to fourth week from dental extraction.10 In a past report, Iizuka et al. reported a case of mandibular fracture following third molar extraction with an infection at the fracture site. Therefore, it is necessary to recognize the possibility that late fracture following third molar extraction can cause osteomyelitis.11 Osteomyelitis of the jaws is usually polymicrobial in nature with Streptococcus, Bacteroides, Lactobacillus, Eubacterium and Klebsiella being the most common offending organisms.12 There has been wide variation in the age spectrum of the reported cases, varying from 14- 82 years with a mean of 40.8 years ± 21 years. No gender specificity has been found with the disease affecting. Risk factors for osteomyelitis of jaw include chronic systemic disease, alterations in the vascularity of bone and compromised host defences like diabetes mellitus, malignancy, malnutrition, acute and chronic anaemias, osteopetrosis, intravenous drug abuse or AIDS. 13 Secondary chronic osteomyelitis is currently considered the most frequent form of osteomyelitis with an incidence of 70% while the incidence rate of acute osteomyelitis is 17% and primary chronic osteomyelitis is 10%14 There are probably several factors responsible for the pathogenesis of the patient’s osteomyelitis. The coronoid process is supplied primarily by the temporalis muscle vessels, unlike the remaining mandible, which receives its major blood supply from the inferior alveolar artery. Continued soft-tissue inflammation could have caused inflammatory exudate to pass through the nutrient or Haversian canals, and/or through the temporalis muscle, to the periosteum, causing thrombosis. Moreover, the facial swelling could have resulted in temporalis muscle compression, which could also disrupt the blood flow to the coronoid process. A combination of these events would be enough to cause vascular collapse and associated venous stasis, and result in ischemic changes in the coronoid process that would predispose to the development of osteomyelitis.15 In our case the occurrence of coronoid osteomyelitis could be followed by the removal of infected third molar.
Conclusion
To conclude, the reason for fracture of the coronoid process could be temporalis muscle pull or compromised vascularity causing the pathological fracture. The literature shows occurrence of osteomyelitis of mandible following third molar extraction the involvement of coronoid process with the disease is very rare. This report presents a case of pathological fracture of coronoid process which lead to osteomyelitis of coronoid process following extraction infected third molar with detailed explanation of surgical procedure performed.