
Introduction
Megaureter often known with other names such as hydroureter, large ureter, wide ureter and megaloureter represents a ureter with a diameter larger than normal with or without associated renal pelvis dilatation.1 Congenital anomalies of the vesico-ureteric junction (VUJ) are often associated with a dilated or megaureter. Smith2 classified megaureters into four categories, obstructed, refluxing, refluxing with obstruction, and non-refluxing/non-obstructing, later subdivided into primary and secondary by King.3 The majority of megaureters can be managed conservatively, however the indications and surgical options in patients requiring intervention are less well defined.
Primary obstructive megaureter is common in children but as a primary presentation is uncommon in adults. It is characterized by an intrinsic congenital obstruction at the lower 1 to 2 cm of the ureter. The diagnostic criteria include (a) dilated ureter as seen on intravenous urography, retrograde pyelography, antegrade pyelography, ultrasonography, or magnetic resonance urography; (b) lower end of ureter ending in a smooth taper; (c) absence of vesicoureteral reflux; (d) absence of infravesical obstruction; and (e) absence of organic obstruction at the lower end of the ureter as confirmed by cystoscopy and ureteral catheterization.4 Obstructive megaureter in an adult has a variable course and mostly present in the third decade of life with reduced function or complications such as secondary calculi, and recurrent infection. In this paper we report a case of primary obstructive megaureter in a 21-year-old male presenting with loin pain.
Case Report
A 21-year-old male presented to the Urological services of our hospital with left loin pain of 2 months duration. He had earlier consulted a local physician for the same and had undergone imaging, both ultrasonography and computed tomography. Ultrasonography revealed a left sided hydroureteronephrosis secondary to distal obstruction (Figure 1). Computed tomography revealed left sided mild to moderate hydronephrosis and dilatation of the entire ureter (Figure 2). The patient was stented on the left side and referred to our hospital for further management.

Figure 2
a. CT shows dilated left pelvis calyceal system. b. CT shows dilated left lower ureter near the bladder.

Figure 3
a. Retrograde pyelogram shows dilated and tortures left lower ureter. b. Retrograde pyelogram shows dilated left lower ureter very narrow terminal 1.5 cm ureter.
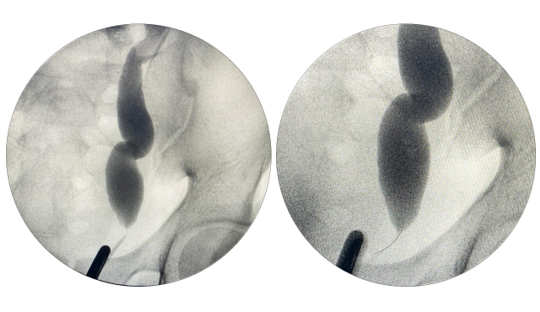
The patient was posted for cystoscopy and left sided ureteropyelogram under general anaesthesia. The ureteric catheter could be easily passed across the left ureterovesical junction. Contrast was injected into the left ureter and ureteropyelography was performed. The whole length of the left ureter was dilated except for the terminal 1.5 cm (Figure 3). There was a smooth tapering noticed at the terminal portion of the left ureter. In view of these findings and taking the patients symptoms into consideration, the patient underwent left sided ureteroneocystostomy.
Post-operative recovery was good. The catheter was removed after 96 hours and the patient voided well. Post-operatively the patient was free of symptoms. Postoperative renogram done 12 weeks after double J ureteric stent removal revealed good drainage.
Discussion
Primary obstructive megaureter is a functional obstruction secondary to an adynamic lower ureteral segment. It may be related to either increased levels of collagen, which lead to fibrosis and obstruction, or atrophy of the inner longitudinal muscle in the distal ureteral segment, which leads to impaired transmission of peristalsis. It can also be due to hypertrophy of the outer compressive circular muscle, also resulting in obstruction. The frequency is about 0.36 of 1000 live births.5 The clinical presentation is variable and depends on the age group, with children presenting with UTI and flank pain and adults commonly presenting with hematuria and urolithiasis.4 Computed tomography and Magnetic resonance urogram findings of primary obstructive megaureter include a dilated proximal ureter associated with a dilated collecting system and gradual smooth tapering of the distal ureter without an associated mass lesion. However, functional imaging with dynamic renography using 99mTc-mercaptoacetyltriglycine is often necessary to correctly diagnose the condition and triage patients to appropriate therapy.6
Primary obstructive megaureter in adults usually presents in the third or fourth decades of life. Men are more commonly affected than women.4 Unilateral disease is more common and is usually on the left side. The disease can present with flank pain, recurrent urinary tract infections, hematuria, and urolithiasis. Renal failure has been described as rare, ranging from 0% to 10%, and the condition in adults has been perceived as having an innocuous course.7 Urolithiasis is known to occur in 12% to 20% of the cases4 although Hemal et al 4 reported that 30.9% of the patients in their series had associated urolithiasis. In view of complications such as urolithiasis, infections and deterioration of renal function, several treatment approaches have been suggested such as excision of the adynamic segment and ureteroneocystostomy with or without tailoring.
To conclude primary obstructive megaureter in adults differs from that encountered in childhood. The growth and maturation of the vesicoureteral junction and the kidney are complete in adults and therefore little spontaneous improvement can be anticipated, unlike that observed in children.4 The degree of dilation of the whole ureter, pelvis, and calices is more common in adult megaureter. The disease process is chronic in nature and that explains the higher incidence of complications, such as secondary urolithiasis and renal failure in adults. This may be because of the late presentation and silent subclinical damage. It is therefore evident that the adult megaureter requires a more aggressive surgical approach than primary obstructive megaureter observed in the pediatric population. Surgical correction relieves obstruction and improves drainage and although renal functional improvement may not be substantial, further deterioration and complications are prevented.